
The Centre of Disease Control (CDC) published the first reports of HIV in 1981, however the advent of combination Antiretroviral Therapy with Protease Inhibitors in 1996 significantly changed the management of HIV/AIDS, with a decline in HIV-related mortality. The healthcare landscape for people living with HIV has improved exponentially over the past 3 decades, whereby treatment has been a spectacular success and now the U=U statement is being endorsed globally; meaning people living with HIV on Antiretroviral Therapy with an undetectable viral load in their blood have a negligible risk of sexual transmission of HIV. Consequently with effective treatment, HIV is considered a chronic condition, and people living with HIV can expect to live normal life expectancies. People are therefore living longer and ageing with HIV or acquiring HIV in older age. With 36.7million people living with HIV globally and over half having access to Antiretroviral Therapy, healthcare services need to prepare for an ageing HIV epidemic, which is largely unchartered territory.
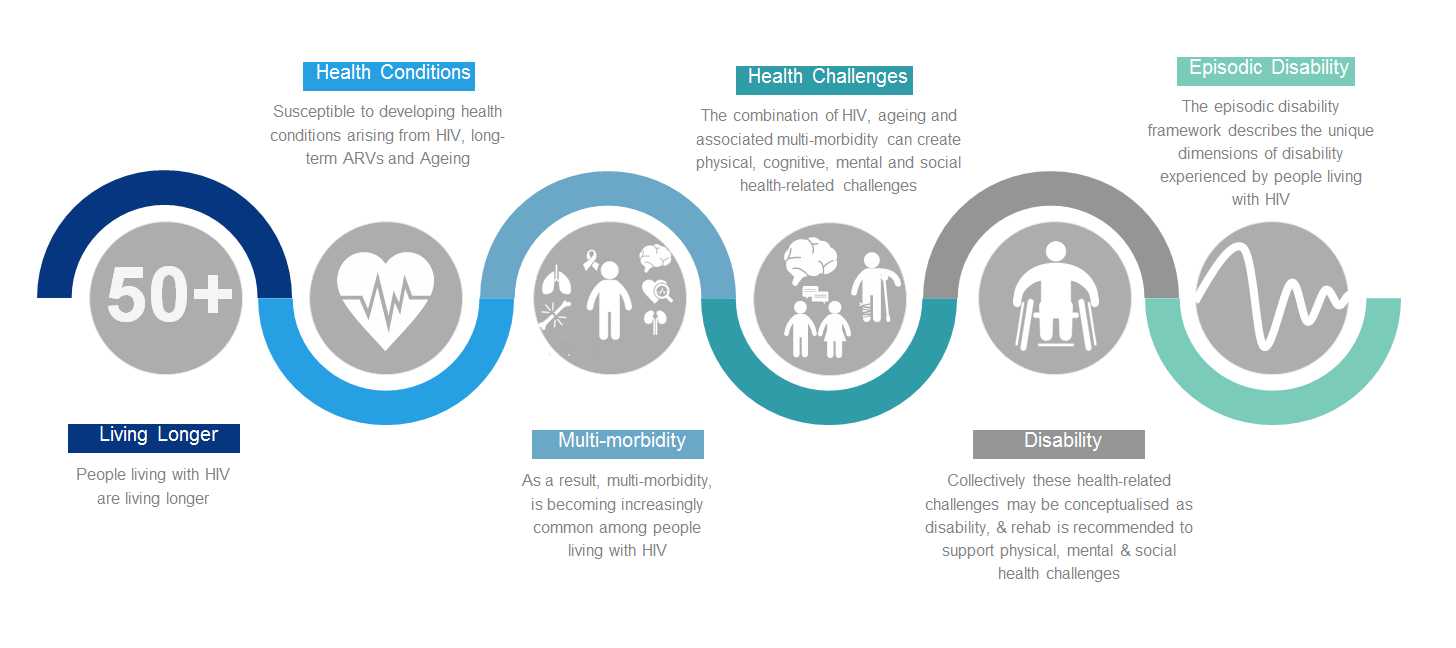
As more people are ageing with HIV, it is estimated by Public Health England that by 2028, over half of people living with HIV in the UK will be 50 years or above. However as people are ageing with HIV, they may be susceptible to developing conditions arising from HIV, adverse effects of long-term Antiretroviral Therapy or ageing, resulting in increasingly more prevalent multi-morbidity; which can create physical, cognitive, mental and social health related challenges. Collectively these challenges may be conceptualised as disability; and rehabilitation is recommended to support physical, mental and social health challenges. The Episodic Disability Framework describes the unique dimensions of disability experienced by people living with HIV, whereby fluctuating or episodic disability experienced, creates periods of wellness that can be interrupted by periods of illness. From this framework the HIV Disability Questionnaire has been developed to measure the presence, severity and episodic nature of disability. Rehabilitation, such as physiotherapy, is recommended to support older adults living with HIV, and aerobic and progressive resistance exercises are safe and effective rehabilitation and self-management interventions. There are educational e-modules to support evidence informed rehabilitation including a version for Sub-Saharan Africa. In addition research priorities for HIV rehabilitation have been clearly established.
However, even though HIV rehabilitation may be highly equitable, it is internationally undervalued. Commonly the usual continuum of care for people living with HIV does not include rehabilitation, such as Physiotherapy, for people who experience disability. There are significant variations in access, service provision and consequently outcomes. Physiotherapy has a crucial role to play in working with people living with HIV and their communities, health and social care providers, educational institutions, and policy drivers to focus on function, ability and inclusion. Whereas Antiretroviral Therapy is bringing years to life, Physiotherapy (and rehabilitation more broadly) is bringing life to years. With the World Health Organisations call for action; Rehabilitation 2030 – it is time that HIV rehabilitation is discussed at a policy level, and its valuable role is recognised in supporting existing care services of people living with HIV.
There are examples of successful and novel HIV Physiotherapy services; such as utilising a “task shifting approach” where Physiotherapists train less qualified staff to complete more complex tasks in resource poor settings; open access models of Hospital outpatient group rehabilitation interventions designed to address episodic disability to reduce barriers and improve accessibility and engagement; and adopting community based exercise programmes to address the emerging needs of people with HIV and multimorbidity.
This regular blog will feature a range of topics that aim to advocate for the important role of Physiotherapy and rehabilitation, address key issues and facilitate knowledge transfer and exchange. Consequently this blog will be relevant to people living with HIV, rehabilitation professionals, clinicians, academics, service providers and policy stakeholders.
No comments:
Post a Comment