
One of my favorite excerpts from an editorial in quite awhile…
Clinicians should quit looking for
overly simplistic answers. Clinical
diagnosis, like producing a great wine,
is complex and requires an appreciation
of the data that can be gathered
within the nuances of patient interaction
I do not think I am alone when we all learned clinical tests, or special tests, in PT school, it was one of the coolest things ever! It was gratifying to go from theory to “practice” and actually be able to diagnose something! Unfortunately, as I continued to learn more, this bubbled busted—and busted with explosive power.
If only it was that easy.
The recent editorial, entitled “Orthopaedic special tests and diagnostic accuracy studies: house wine served in very cheap containers” in BJSM by Hegedus/Wright/Cook (free to access) brings to light the errors associated with clinical diagnostic tests with overall intention of clinicians to utilize clinical reasoning on refined data.
We have these special tests for cervical vertigo / cervicogenic dizziness–i.e. joint position error testing and cervical torsion tests, to aid in our hypothesis—but unfortunately, just like diagnostic tests to rule in hip/shoulder impingement and meniscal tears–these are limited.
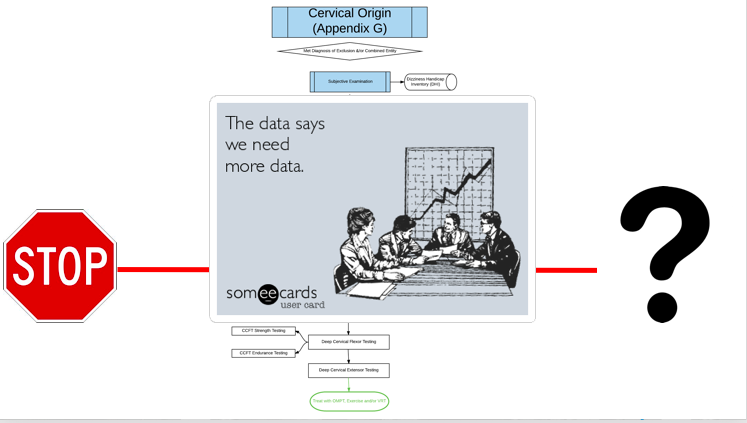
So when you ask someone about the diagnosis of Cervicogenic Dizziness—back away if he/she quickly throws at you Joint Position Error Testing—even though this is promising, we are better than that. We should be better than that. JPE testing will simply add more data to the already established data. The already established data is a stronger foundation, a safer foundation, for your clinical examination.
I have spent the last few years of my clinical career examining every article published (in multiple languages!) coupled with clinical practice to provide the most optimal diagnostic process to put together my Optimal Sequence Algorithm. In my personal opinion, I think this diagnosis is the most controversial (besides SIJ!), but ultimately takes the gold medal in clinical reasoning due to the often, and intimidating, nature of dizziness in non-benign conditions, including vascular and other central disorders. No one should be comfortable jumping into the upper neck with someone experiencing dizziness without sound judgement and training.
As previously quoted, “clinicians should stop looking for overly simplistic answers”. Let me help guide your thought process in this unnerving and overwhelming part of the human body. These patients are walking in your door—let me help you get them better.
My next course is in Richmond, VA on November 4-5, 2017. Sign up by midnight tonight---October 5, 2017--- for a $100 Discount!
You can learn more about the screening and treatment process of Cervicogenic Dizzinesss throughIntegrative Clinical Concepts, where the author and his wife, a Vestibular Specialist, teach a 2-day course. Pertinent to this blog post, the first day provides the most up-to-date evidence review from multiple disciplines to diagnose through the “Optimal Sequence Algorithm” to assist in ruling out disorders and ruling in cervical spine, including determining if single or double entity exists.
If you would like to host a course for your staff (either a vestibular, neuro, sports or ortho clinic), please do not hesitate to contact me at harrisonvaughanpt@gmail.com for prices and discounts.
Authors
Harrison N. Vaughan, PT, DPT, OCS, Dip. Osteopracic, FAAOMPT
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts
Danielle N. Vaughan, PT, DPT, Vestibular Specialist
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts


Want an approach that enhances your existing evaluation and treatment? No commercial model gives you THE answer. You need an approach that blends the modern with the old school. Live cases, webinars, lectures, Q&A, hundreds of techniques and more! Check out Modern Manual Therapy!
Keeping it Eclectic...

No comments:
Post a Comment